12 Leads ECG and 10 leads ECG Cable
This passsage Comprehensive introduce the factors that will influence the 12 leads ECG,and provide useful tips on different angles.Especially some cases other article seldomly mentioned,such as ECG on Female patient,unconcious patient,on children and neonata.
What is more,it provide some possible solving ideas from the upstream of ECG,i.e ECG leads cable/Patient cable manufacturer
12 leads ECG/EKG Interpretation
12 leads ECG System
The 12-lead ECG is used to trace the heart muscle from 12 different electrical positions. Every electrode will seize the electrical activity from a different position. So that an experienced interpreter will see the heart from different angles and make accurate diagnosis.
The heart’s electrical signals are detected by electrodes sticking to the appointed positions on the skin.
During the past century ,different leads systems were developed out, such as Einthoven’s Lead System,Goldberger’s Lead System,Wilson’s Lead System,Frank’s Lead System,EASI Lead System,360°Lead System. The 12 lead ECG system is the commonest ECG system today, A 12-lead ECG integrates the advantages of Einthoven’s Lead System,Goldberger’s Lead System and Wilson’s Lead System. The 12 leads ECG can monitor all heart activities, both rhythmic and ischemic abnormalities on the anterior heart wall. So it is regarded as the platinum standard for ECG diagnosis before 15 leads ECG system and 18 leads ECG system. However, it is still the most widely used ECG diagnosis.
12 leads ECG has only 10 electrodes-Why
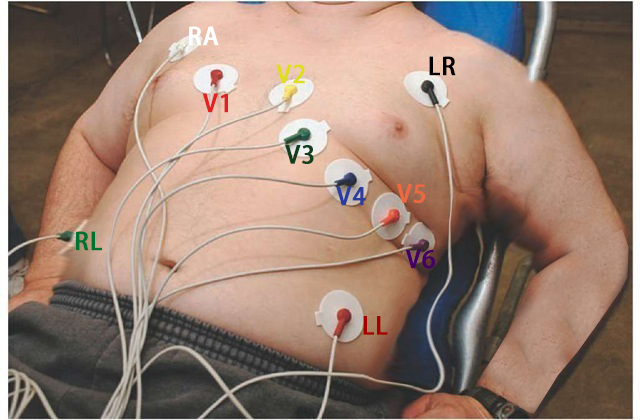
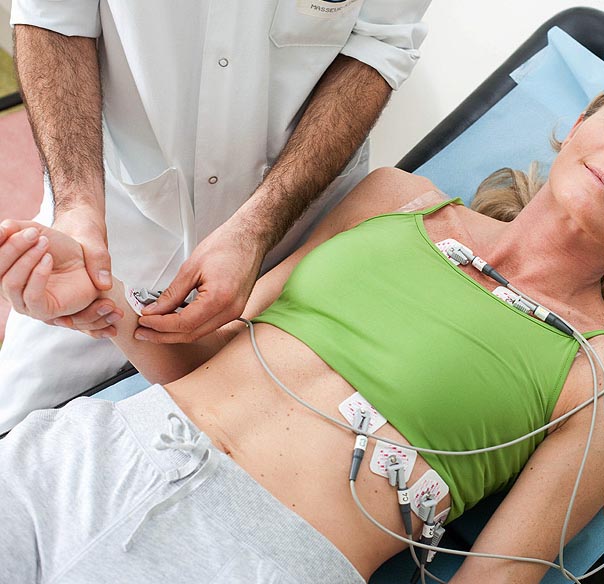
12 lead ECG lead/electrodes application
12 lead holter monitor
24-hours Holter monitoring is used to record patient heart’s rate and rhythm continuously for 24 hours or Longer.. Patient will wear the Holter monitor for 12 to 48 hours. ECG Holter Recorder also has electrodes and electrical leads as ECG does, but with less electrodes. It record not only heart’s rate and rhythm but also pick up the signal when patient are suffering chest pains or exhibiting symptoms of an arrhythmia (irregular heartbeat )
12 lead ECG monitor
12-lead ECG will help EMS doctors to fast identify STEMI/heart attack patient and filtrate patients for possible cardiac ischemia..
Useful tips for Optimizing 12 leads ECG
The heart’s electrical signal has very little output, so it can easily be combined with other signals of identical frequency to create artifact. It is not uncommon to have some form of artifact for a 12-lead ECG placement but it’s important to attempt to lessen any interference in order to ensure an accurate EKG.
The good news is that there are some measures we can take to reduce artifact as possible as we can,from the level of ECG accessories manufacturer and ECG Operator/Clinicians.
To ECG placement Operator/Doctor
- Place understanding in a recumbent position if the patient will endure.
- Place the patient’s arms somewhere near their side to loosen up their shoulders.
- Patient’s legs ought to be uncrossed.
- Electrical gadgets, for example, cell phones ought to be away from the patient as these gadgets may meddle with the machine.
- Dry the skin on the off chance that it is diaphoretic or clammy.
- Shave any hair that can meddle with terminal situation.
- Electrode gel ought to be wet.
- Electrodes ought not be set over bones and over territories where there is a great deal of muscle development.
- Sometimes a grating material, for example, a wash fabric may should be utilized to evacuate dead skin cells.
To ECG accessories Manufacturer
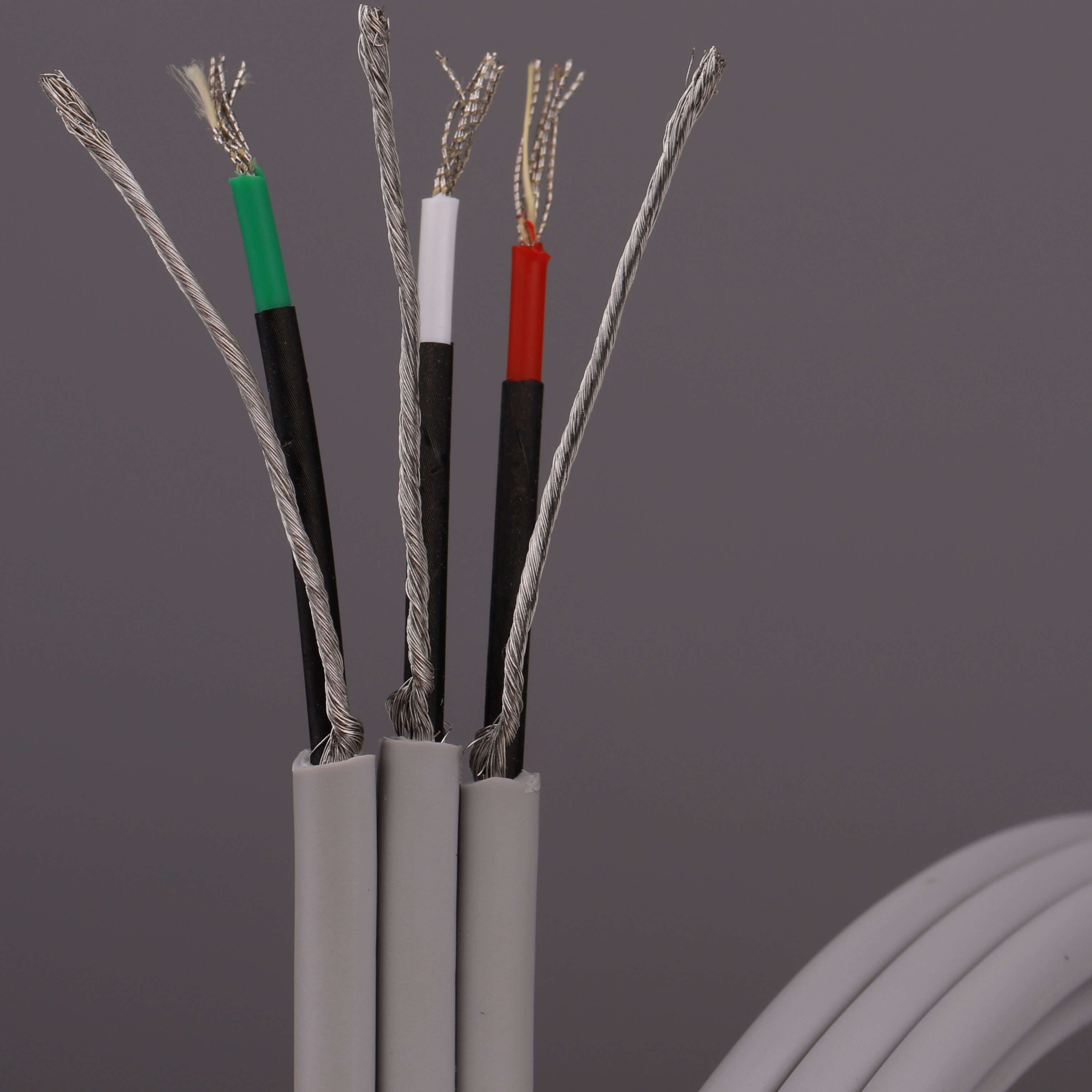
Know how to choose Raw ECG cable
As Heart’s electronic signal is weak,and not all patient can keep a absolutely silent state,but Triboelectric Noise inevitably occurs , Triboelectric Noise in an ECG or other medical signal may make accurate diagnosis difficult or even impossible.So when ECG cable manufacturer are making the ECG cable,the raw cable(single leadswire and trunk ECG cable) Should have very Low Noise performance
Raw ECG cables are all with Shielding to decrease Triboelectric Noise.Generally these shileded ECG raw cables divided into two types:
Cores Individually shielded(which is better)
Cores bulking shielded
Please refer to following blog to find more information
Following Low Noise ECG trunk cable maybe enlightning to you:
12 leads ECG placement
12 lead eCG Placement tutorial video
In order to promote excellence in the recording of in hospital, whilst it is recognized that 12 lead ECGs are performed in a variety of contexts environments and degrees of urgency.
To achieve the best practice, standard electrode positioning should always be made, and the operator must be competent in the use of the ECG machine and in the recording of an ECG ideally this should be demonstrated by the possession of a recognized qualification such as those awarded by the sc/st .It is essential that competence in the recording of an ECG be maintained, and this should be demonstrated by periodic review .
The goal of good scientific practice is to ensure that the patient has a positive experience of the procedure. Good communication skills are a key part of enhancing the patient’s experience of the procedure .As a minimum before any contact with the patient, operators should introduce themselves and explain their job title and role.
They should give a brief description of the procedure for recording an ECG, which should cover the level of undress involved the use of adhesive electrodes and reassurance the procedure is brief and painless. A verbal confirmation of consent is also required. To continue, operators should make every effort to respect the cultural sensitivities of the patient, and try to minimize embarrassment.
Many patients will feel uncomfortable being touched on their upper torso, operators must be sensitive to this and act in a sympathetic caring, and compassionate manner in accordance with the General Medical Council Recommendations .A patient should always be given the option to have a chaperone present, the chaperone must be a health professional with knowledge of the standard practice of recording a 12-lead ECG .
Patients may also request a relative or carer to be present as far as possible. The area in which the ECG is recorded should be private, it can be walled curtained or screened off. It should be quiet, comfortable and accessible for disabled and able-bodied for patients and staff.
It should be safe and clean with appropriate hand cleaning, and clinical waste facilities such as a yellow or orange bag and a sharps container .It should be furnished with a height adjustable couch or bed that can be accessed from both sides. Both the area and the ECG trolley should be stocked appropriately with ECG paper, electrodes, razors tape, alcohol skin wipes gauze, personal protective equipment and machine cleaning wipes.
The electrocardiograph must meet or exceed IEC standards to avoid distortion of the st-segment.
The low frequency cutoff should be no higher than 0.67 Hertz in auto mode or 0.05 Hertz in manual mode to prevent the loss of high frequency information.
The high frequency cutoff should be no lower than 150 Hertz in adults and 250 Hertz in children.
The disposable tab electrodes should all be of the same maker or type and meet or exceed the requirements of current guidelines.
The ECG machine should have a medical physics Electrical Safety sticker on it, which should be in date. The ECG machine should have the correct date and time on it.
The room and equipment should be clean and orderly with all waste from previous investigations disposed of as clinical waste. All main leads cables, wires and connectors should be intact with no evidence of fractures faults or insulation damage.
The ECG machine battery will need to have sufficient charge, a distinguishable plug is useful. If the machine is to be used in sensitive environments, for instance, intensive care units (ICU) where a number of items of vital equipment are all plugged into wall sockets.
Measures to control the risk of infection must be taken in accordance with local policy.
The hands should be washed with soap and water or cleaned with alcohol gel before and after. Any contact with a patient, personal protective equipment should be worn if necessary. Appropriate clinical waste disposal facilities should be available, in the form of an orange bin liner and a sharps bin.
It is essential that the patients are correctly identified, and that the appropriate identifying details are displayed on the screen for patients unable to provide their own identifying details because of ,for instance, unconsciousness.
Confirmation of identity must be sought from carers or by using hospital wristbands.
The printed recording must always be checked to ensure it has the correct patient details.
You now trust consent must be gained from the patient, and in some instances, written consent may be needed. Written consent is also required in the case of an unconscious or confused patient although in a medical emergency.
Overruled a semi-recumbent position of approximately 45 degrees to the horizontal is recommended, any variation from this position should be noted on the ECG, the limbs should be supported by the bed or couch ,and the head and neck supported by a pillow to minimize any artifact caused by muscle tension.
Skin preparation is often required to produce an artifact free ECG. Care must be taken with patients who have sensitive or broken skin.
Various methods are available to minimize the skin to electrode impedance, this includes:
Washing with mild soap and water;
Cleaning with alcohol wipes of exfoliation if this is required.
It should be undertaken with very light abrasion using a paper towel gauze swab or abrasive tape that is designed for this purpose.
Chest hair may need to be removed, oral consent from the patient should be gained .And an unused razor should be employed and disposed of in a sharps bin immediately afterwards.
Electrodes must be positioned in accordance with the AAHA recommendations .If any electrodes need to be cited in non-standard positions, the recording must be labeled with this
Information to avoid misinterpretation of any altered ECG waveforms.
Limb electrode should be placed on the wrists and ankles whenever possible. Moving the electrodes up the limbs may alter the appearance of the ECG, and should be avoided unless there is a significant tremor of a limb or it has been amputated.
Limb electrodes must not be placed on the torso since this cord
is significant alteration to the wave amplitudes. This can invalidate the use of the recording for many diagnostic purposes.
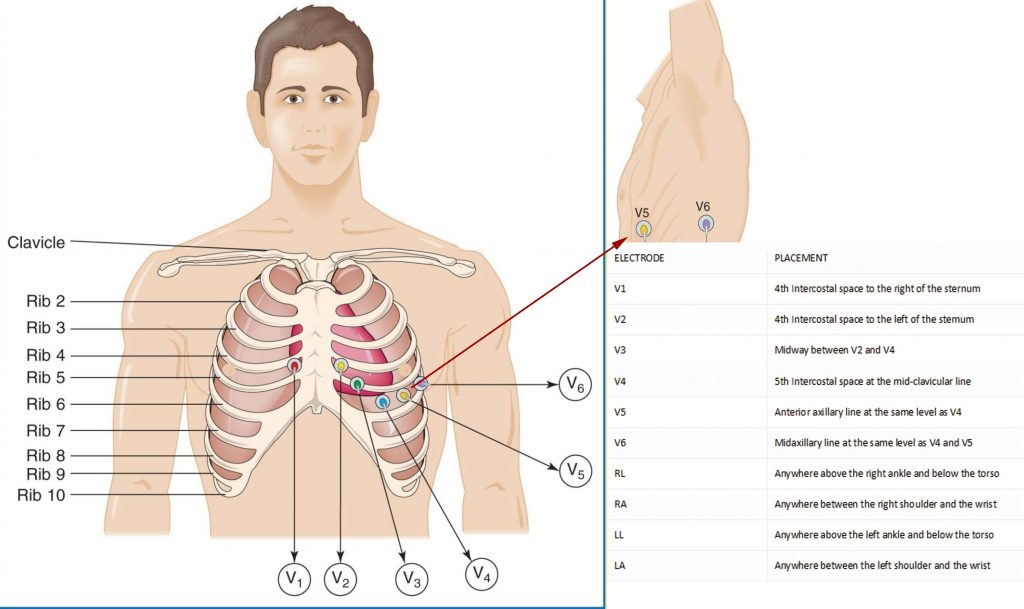
The correct anatomical positions for the chest electrodes have been defined, and must always be used unless it is not possible.
The center of the active area of electrodes should be aligned with the relevant anatomical landmark.
Care should be taken when counting the intercostal spaces from the clavicle, the small space between the clavicle and the first rib is not the first intercostal space. In order to avoid this common
error ,the manubrium joint sometimes( also called the angle of Louie )should be used as the main reference point.
To locate the angle of Louie, a finger should be run down the sternum from the top until a bony horizontal ridge is met.
Sliding the finger down into the right side will locate the second intercostal space from here(find video instruction on the youtube).It is possible to count down to the third and fourth intercostal spaces.
Slide the finger toward the sternum until the edge is felt and place the electrode for v1 in this position. This procedure should be repeated on the left side to correctly position.
The v2 electrode note that the left and right sided rib spaces may be offset so operators should avoid placing v2 adjacent to v1 without counting the rib spaces.
Next the v4 electrode should be placed in the fifth intercostal space in line with the midpoint of the clavicle.
The v3 electrode should then be placed midway between the v2 and v4 electrodes.
The v5 and v6 electrodes should then be positioned in horizontal alignment with the v4 electrode .The v5 electrode should be placed on the anterior axillary line while the v6 electrode should be placed on the mid-axillary line.
When recording an ECG from female patients, it is conventional to place v4 v5 and v6 electrodes beneath the left breast.
When breast tissue overlying the correct anatomical positions, there is some evidence to suggest that the positioning of these electrodes over the breast may not significantly attenuate the signal, but further supporting evidence is needed.
To warrant a change in this recommendation when lifting the breast to place electrodes, care and sensitivity is required, using the back of the hand to lift the breast can be helpful in minimizing contact in order to achieve accurate ECG electrodes positioning.
It is usually necessary for all upper torso clothing to be removed.
Time should be taken to ensure that the patient is relaxed and comfortable.
An ECG with somatic muscle interference is more difficult to interpret, some patients cannot fully relax due to pain from arthritis or other conditions such as Parkinson’s disease which may cause a resting tremor. These patients should be made as comfortable as possible.
And the ECG trace annotated with an appropriate explanation on occasion. It may be necessary to adapt the ECG recording techniques, for example, when a patient is sitting in a wheelchair, when a patient is lying flat,or when a patient is sitting upright in bed because of respiratory difficulties.
Any variations to the standard recording techniques should be described in writing on the recording. The appropriate buttons should be pressed to initiate a new ECG. This button is usually labeled as start auto or ECG a 12-lead ECG.
And simultaneous rhythm strip is most commonly recorded at 25 millimeters per second with a gain setting of 10 millimeters per mini volts. The initial recording should be made without the use
of the manual filter, which alters the upper cutoff frequency to 40 Hertz. The filter will reduce interference but it also distorts the ECG and should only be used when absolutely necessary and when all other attempts to eliminate artifact have failed. If despite efforts to relax the patient and make them comfortable,
there is still somatic muscle interference on the ECG, the filter maybe switched on ,and the recording repeated use of the filter should be clearly indicated on the final ECG printout incorrectly .pressing copy or reprint may on some ECG machines.
Initiate a printout of an ECG from a previous patient if patient details are not entered into the Machine, it may not be clear that this ECG relates to a previous patient, therefore operators must fully understand the equipment they are using, and the potential consequences of mistakes. If the ECG complexes are of such high amplitude that they overlap then the game may need to be adjusted to 5millimeters per millivolt to enable clearer visualization of the complexes,and more accurate measurements to made. Any alteration to the game setting should be clearly marked on the ECG. Any features on the ECG that might indicate
the need for urgent medical attention should be brought to the attention of appropriate staff. If the patient has any symptoms of possible cardiac origin, such as “chest pain, palpitation or dizziness” at the time of the recording, then this should be written on the ECG. The recording should be of good quality, and
should be assessed to ensure that all waveforms such as p-waves ,QRS complexes,and T waves are clearly visible; the isoelectric line which is the baseline between each ECG deflection should be stable and not wandering ,and it should be free of interference. The ECG should be correctly labeled with the patient’s identification and any relevant clinical details as well as any adjustments made to the recording.
Dextrocardia is the most calm form of cardiac malposition, and refers to any situation where the heart is located within the right side of the chest rather than the left. It may be associated with the condition situs inversus where other internal organs are in a mirror-image relationship to the usual position.
Dextrocardia may be suspected if arresting 12-lead ECG has negative P waves and QRS complexes in lead 1 in the absence of any technical error, such as “reversal of the right and left arm connections, poor R wave progression observed in leads v1 through to v6” would also support this interpretation. In this case a second ECG should be recorded with the chest electrodes v3 to v6 positioned on the right side of the chest using the same intercostal spacing and anatomical landmarks as previously described. But this time on the right side v1 and v2 should remain in their usual positions. This approach should provide a true ECG representation. In such a case, the limb lead complexes in lead 1 will continue to appear inverted demonstrating the abnormal location of the heart, however the reposition leads v3 to v6 will now show appropriate R wave progression, and there should be clear annotation on the recording to describe the repositioned electrodes in such a case by using, for example, V3R, V4R, V5R and V6R.
An alternative approach is to swap the right and left arm connections. This will normalize the appearance of the limb leads. If this approach is preferred, it is imperative that the ECG be clearly annotated to prevent the possibility of dextrocardia being overlooked.
In some clinical situations, the recording of posterior electrode positions may be necessary posterior electrodes are placed in the same transverse plane as v4; v7 or c7 is placed in the left posterior axillary line, at the same horizontal level as v4; v8 or c8 is placed in the left mid scapular line at the same horizontal level as v4 v; V9 or c 9 is placed along the left spinal border at the same horizontal level as Lead v4.
In the absence of an ECG machine with the ability to record a 15 lead ECG, it is recommended that a standard 12 lead ECG is recorded first subsequently.
V4, V5 and V6 should be repositioned as V7 V8 and V9 ,and a second recording made showing these posterior leads, the second recording must be clearly annotated with the new lead positions right-sided. Posterior electrode positions are locating the same anatomical positions but on the right side, and are then annotated V7R, V8R and V9R.
when recording an ECG on children, it is recommended that the technique be adapted to meet the requirements of the child.
A patient and gentle approach is recommended to attain an artifact free ECG tracing. The recording method is similar to that described for adults. If possible the recording should be made with the child semi-recumbent, but the sitting position may be used if this will prevent restlessness or distress.
The forelimb electrodes are attached as previously described ;the chest electrodes are normally positioned as previously described, but additional leads such as V4R V5R and V7R may be recorded at the request of a clinician,or according to local policy.
Whilst practice is variable in the routine, leaves use of right-sided chest leads
When recording ECGs on children, it is not uncommon to find V4R used in infants up to 1 year old, practice is determined largely by the indications for the ECG and clinician preference. In
some hospital if the child’s chest is not large enough, so that all six chest electrodes can be placed in their standard positions without overlapping, then electrode V3 should be removed and
placed in the fifth intercostal space in the midclavicular line on the right side, and this now therefore becomes V4R. By doing this ,enough room is created on the left side of the chest to allow the other electrodes to be placed in their correct anatomical positions without having contact with each other.
This alteration to the standard technique is normally needed in neonatal department.
The ECG should be clearly annotated with any changes if this technique is used.
In conclusion, to be of maximum diagnostic value, an ECG must be recorded correctly by paying proper attention to patient, preparation, electrode positioning and the other factors described in this article. This is not difficult to do and it is hoped that widespread adoption of this guidance will help to ensure a uniformly high standard of practice in ECG recording with consequent benefits to patient care everywhere you are trusted in.